-

Join Dr. Levy for a six-hour virtual workshop called "Optimal Treatment of Disease with Dr. Thomas Levy" on how what protocols to use to optimally treat disease on February 26, 2023
Read More -

What is a root canal treatment and could this be the cause of chronic disease? Such a treatment, typically just called a "root canal," refers to a dental procedure commonly performed today on a badly decayed or infected tooth, and are an overlooked cause of chronic disease, often with the patient presenting with pain.
Read More -
A question that has been presented to me numerous times since the publication of my book, Curing the Incurable: Vitamin C, Infectious Diseases, and Toxins, is "What kind of vitamin C should I take, and why?" It is a very good question, indeed, as the variable effects on both short-term and long-term clinical outcomes can be dramatic.
Read More -
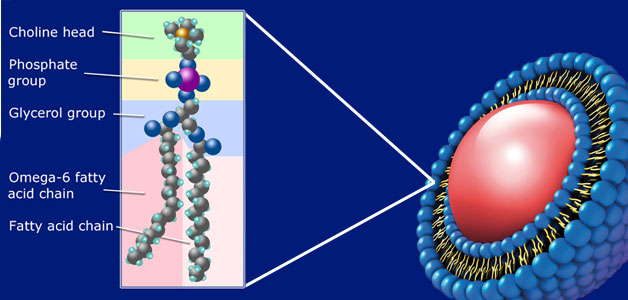
Phospholipids are the primary building blocks of cellular membranes. These membranes are the "containers" that hold the living matter within each cell. They also give definition, shape, and protection to many of the substructures (organelles within the cell like the nucleus and mitochondria) within our cells.
Read More -
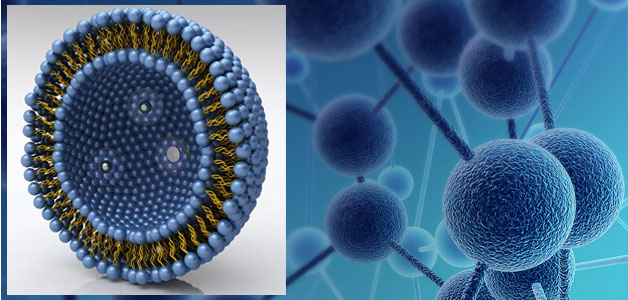
Liposomes are bilayer (double-layer), liquid-filled bubbles made from phospholipids. Over 50 years ago, researchers discovered that these spheres could be filled with therapeutic agents and used to protect and deliver these agents into the body and even into specific cells of the body.
Read More
Health Articles

Thomas E. Levy, MD, JD
Dr. Thomas E. Levy is a board certified cardiologist and has written six books on health-related issues. Most of his work has centered on how to restore and maintain good health in the face of the many different forms of toxicity that all of us face, typically on a daily basis. He no longer has a clinical practice of medicine and cardiology. Rather, he limits himself to research and writing at this time, and he is currently working on his seventh book, Death by Calcium: The Supplement that Kills.
Appearances

Dr. Levy on Extreme Health Radio
The Extreme Health Radio show hosted Dr. Tom Levy on a recent episode of the program. In this program, the audience was told about the power of liposomal vitamin c and why homemade liposomal vitamin c may not be the best. Dr. Levy also spoke about iron, and why it is dangerous, dental health, detoxification and much more!